
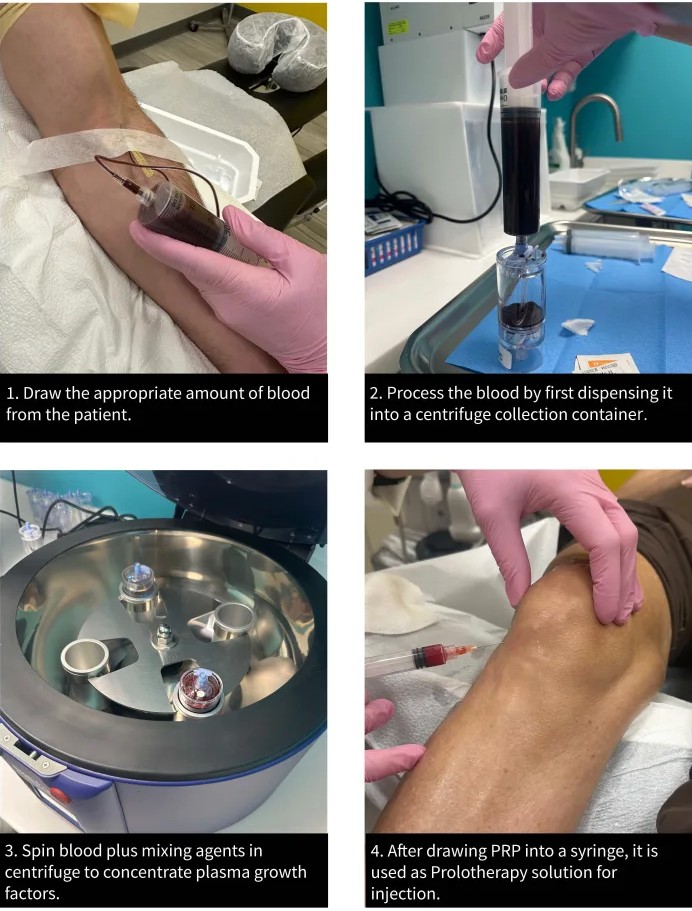
Platelet-rich plasma (PRP) is made from your own blood. A small sample is taken and spun in a centrifuge to separate and concentrate the platelets — the blood cells that release growth factors involved in healing. The concentrated plasma is then injected into the painful area, such as an arthritic knee or an injured tendon, with the aim of reducing pain and supporting the local healing environment.
PRP has become popular for joint and tendon problems, but it sits in an honest grey zone: it is not a proven cure, the preparations and protocols vary widely between clinics, and the quality of evidence differs by condition. It is best understood as an option to consider when standard measures have not been enough, chosen with realistic expectations — not as a shortcut past exercise, weight management and the other foundations of joint care.
PRP is a treatment, not a condition, so the relevant question is which problems it is used for. The conditions where PRP is most often considered in orthopaedics include:
PRP is generally less useful in advanced, bone-on-bone arthritis, where the structural damage is beyond what any injection can address, and where the conversation is usually about surgery instead.
The rationale for PRP rests on biology: platelets release growth factors that participate in tissue repair and modulate inflammation. Concentrating and delivering them to a damaged joint or tendon is intended to shift the local environment towards repair and away from painful inflammation.
The honest caveat is that biological plausibility is not the same as proven benefit. Cartilage that is already worn is not regrown by PRP, and the degree to which PRP changes the natural course of arthritis is uncertain. What some studies do suggest is a reduction in pain for a period in selected patients with earlier arthritis — an effect on symptoms rather than a reversal of the disease.
PRP is an elective treatment, so there is no urgency to it. See a doctor to discuss whether PRP is reasonable if you have joint or tendon pain that has not settled with core treatment and you are considering your options.
Seek prompt care instead — not PRP — if you have red flags: a hot, red, swollen joint with fever (possible infection), sudden inability to bear weight, or a joint that is rapidly worsening. These need diagnosis and treatment in their own right; an injection is not the answer to an undiagnosed acute problem.
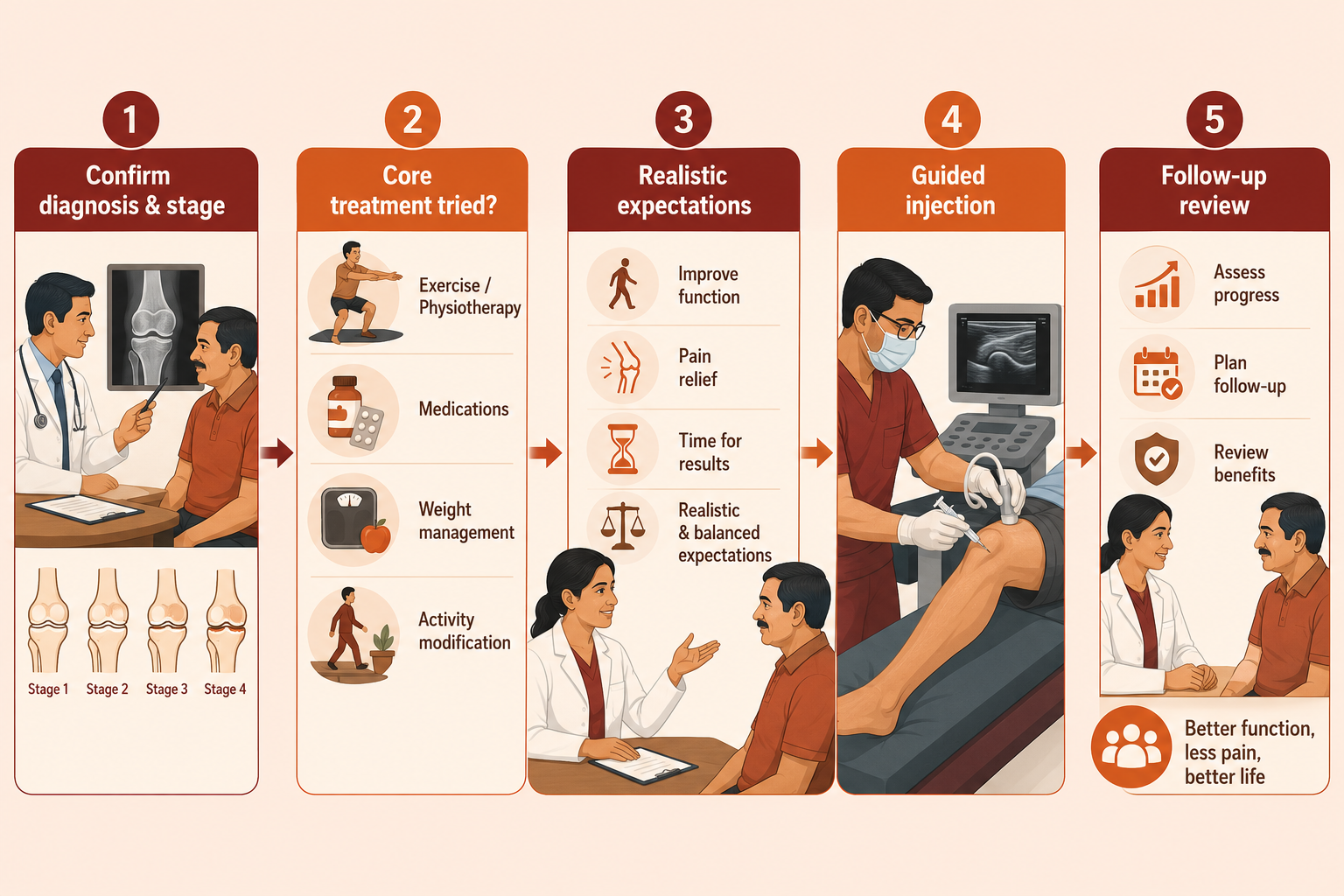
Before offering PRP at VinayakM, we establish that it is a sensible choice for you:
This assessment is where we give you an honest view of the likely benefit for your specific situation.
The procedure:
The whole process usually takes under an hour and is done as an outpatient. Some soreness at the site for a few days afterwards is common; you may be advised to avoid anti-inflammatory painkillers for a period, as they may counteract the intended effect.
Number of injections and results: protocols vary — some use a single injection, others a short course. If PRP helps, benefit tends to build over weeks rather than immediately, and any effect is usually temporary, potentially repeatable. There is no guarantee of benefit.
Honest evidence: for mild-to-moderate knee osteoarthritis, some studies suggest PRP can reduce pain, in places outperforming certain other injections, but the evidence is inconsistent and preparations are not standardised, so guidelines stop short of a general recommendation. For some tendinopathies, evidence is similarly mixed. PRP does not regrow cartilage or cure arthritis. Because it is usually a self-funded treatment, the realistic likelihood of benefit and the cost are both part of the decision.
Alternatives include continuing structured exercise and weight management, corticosteroid or hyaluronic acid injections, and — for advanced disease — surgery. We compare these with you; see also PRP vs hyaluronic acid.
At VinayakM in Greater Kailash-1, PRP is offered by Dr Udit Vinayak (trauma, sports medicine and joint replacement surgeon) as one considered option — never a sales pitch. Our approach:
If PRP is unlikely to help your knee, we will say so.
PRP is a treatment, so 'prevention' here means protecting the joint or tendon so that you rely less on injections in the first place:
It is made from your own blood. A small sample is drawn and spun in a centrifuge to concentrate the platelets, which release growth factors involved in healing. This concentrated plasma is then injected into the painful joint or tendon. Because it comes from your own body, allergic reactions to the material itself are not a concern.
No. PRP does not regrow worn cartilage and does not cure arthritis. In selected patients with mild-to-moderate arthritis, some studies suggest it can reduce pain for a period, but that is an effect on symptoms, not a reversal of the disease. Be cautious of any clinic claiming otherwise.
Protocols vary — some use a single injection, others a short course. If PRP helps, the benefit usually builds over several weeks rather than immediately, and any effect tends to be temporary and potentially repeatable. There is no guaranteed response, which is part of what we discuss beforehand.
Because PRP uses your own blood, it is generally well tolerated. The main effects are temporary soreness or swelling at the injection site, and, as with any injection, a small risk of infection or bleeding. It may be unsuitable if you have certain blood conditions or an active infection. We check suitability before proceeding.
It depends on the situation and the evidence is mixed. Steroid injections act quickly but briefly; hyaluronic acid and PRP are sometimes used for longer-term symptom relief in earlier arthritis. No injection suits everyone. We compare the options for your specific knee — see our page comparing PRP and hyaluronic acid.
