
Healthy joints contain synovial fluid rich in hyaluronic acid, a substance that helps the joint move smoothly and cushions it against load. In osteoarthritis, this fluid becomes thinner and less effective. Viscosupplementation aims to top up the joint with a hyaluronic-acid preparation to restore some lubrication and cushioning, and possibly to calm inflammation, reducing pain.
Like PRP, hyaluronic acid injection sits in an honest grey zone. It is not a cure and does not regrow cartilage; it is a way of trying to ease symptoms in the right patient at the right stage. Views among experts and guidelines genuinely differ on how much it helps, which is why the decision should be individual and based on realistic expectations rather than marketing.

As a treatment, the relevant question is which knees it is used for. Hyaluronic acid injections are most often considered for:
It is less likely to help in advanced, bone-on-bone arthritis, where structural damage dominates and the discussion usually turns to surgery. It is used mainly in the knee, though it is sometimes tried in other joints.
The rationale is mechanical and biochemical. In osteoarthritis the natural hyaluronic acid in joint fluid is reduced and degraded, so the fluid lubricates and cushions less well. Injecting a hyaluronic-acid preparation aims to temporarily restore these properties and may have mild anti-inflammatory effects.
The honest caveat, as with any injection for arthritis, is that this addresses the joint environment and symptoms, not the underlying loss of cartilage. Any benefit is therefore about comfort and function for a period, not a change in the structural disease.
This is an elective treatment, so there is no urgency. See a doctor to discuss whether viscosupplementation is reasonable if knee arthritis pain persists despite core treatment and you are weighing your options.
Seek prompt care instead — not an injection — for red flags: a hot, red, swollen knee with fever (possible infection), sudden inability to bear weight, or a rapidly worsening knee. An injection is never the right response to an undiagnosed acute joint problem.
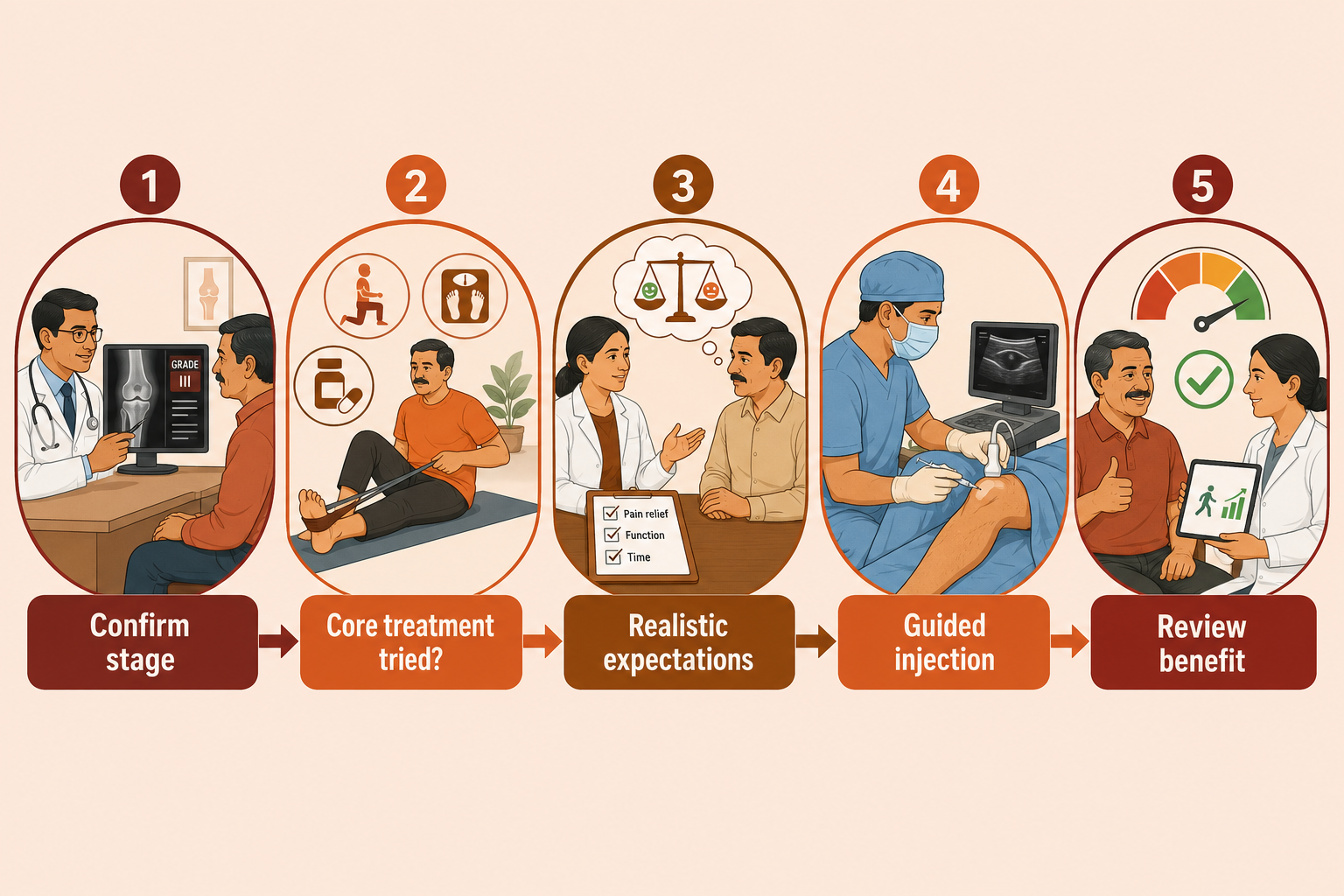
Before offering hyaluronic acid injections at VinayakM, we make sure it fits:
This is where we give you a candid view of how likely it is to help your knee, and how it compares with the alternatives.
The procedure:
It is an outpatient procedure. Mild soreness or swelling for a day or two is common; heavy activity is usually avoided briefly afterwards.
Results and honest evidence: if it works, relief tends to build over a few weeks and may last several months, after which it can be repeated. However, the evidence is genuinely mixed — some studies and patients report worthwhile relief in earlier arthritis, while large reviews find the average benefit modest, and major guidelines differ, with some (such as NICE) not recommending it routinely. It does not cure arthritis or regrow cartilage. Because it is often self-funded, the realistic chance of benefit and the cost both matter in the decision.
Alternatives include continued exercise and weight management, corticosteroid injections (faster but shorter-acting), PRP injections, and — for advanced disease — surgery. See PRP vs hyaluronic acid for a direct comparison.
At VinayakM in Greater Kailash-1, viscosupplementation is offered by Dr Udit Vinayak (trauma, sports medicine and joint replacement surgeon) as one option among several, chosen honestly:
Where the injection is unlikely to help, we will tell you and discuss better-suited options.
Because this treats symptoms rather than cause, the durable work lies in protecting the joint:

It is an injection of a gel-like fluid similar to a natural component of healthy joint fluid, given into an arthritic knee to improve lubrication and cushioning and ease pain. It is also called viscosupplementation. Depending on the product, it is given as a single injection or a short weekly course.
When it helps, relief usually builds over a few weeks and may last several months, after which it can be repeated. Responses vary widely — some people notice a worthwhile difference, others little. It does not cure arthritis; any benefit is temporary symptom relief.
The evidence is mixed. Some studies and patients report useful relief in mild-to-moderate arthritis, while large reviews find the average benefit modest, and guidelines differ — some do not recommend it routinely. It is reasonable to consider in selected patients after core treatment, with realistic expectations, but it is not a cure.
They work differently. Steroid injections tend to act quickly but for a shorter time and are useful for flares; hyaluronic acid may act more slowly but potentially last longer in earlier arthritis. Neither suits everyone. The best choice depends on your knee, your stage and your goals, which we discuss individually.
It is generally well tolerated. The common effects are temporary soreness or swelling in the knee for a day or two. As with any joint injection, there is a small risk of infection or bleeding. It is avoided if there is active infection around the knee or a relevant allergy. We check suitability first.
