
Knee replacement (knee arthroplasty) is one of the most successful operations in modern medicine: for the right person, it reliably reduces arthritis pain and restores function. But it is major surgery with a real recovery period and genuine risks, and it is not the first answer for knee arthritis — it is the answer when good non-surgical care has been tried and is no longer enough.
The decision is rarely black and white. It rests on how much the knee is affecting your life, weighed against your general health, your goals, and what surgery can realistically deliver. This page explains when replacement is worth considering, what should be tried first, and how the decision is best made — so you can have an informed conversation rather than a rushed one.
The features that point towards considering a knee replacement are usually a combination, not a single sign:
If pain is intrusive but you have not yet completed good non-surgical treatment, that is usually the place to start rather than surgery.
The overwhelming reason for knee replacement is advanced osteoarthritis — cartilage worn to the point where bone rubs on bone in one or more compartments of the knee (see knee osteoarthritis). Less commonly, replacement is considered for:
What these share is structural joint damage that cannot be undone and that is now overwhelming the knee's function. Replacement addresses the worn surfaces; it does not treat pain coming from other sources, which is why an accurate diagnosis matters before surgery is considered.
Book an orthopaedic assessment if:
And seek prompt care for red flags unrelated to routine arthritis — a hot, red, swollen knee with fever (possible infection), sudden inability to bear weight, or rapidly worsening pain — which need assessment in their own right before any elective surgery is planned.
Deciding about knee replacement is a careful, unhurried assessment at VinayakM:
The output is not just "yes or no" but "what is the best next step for you, and when".
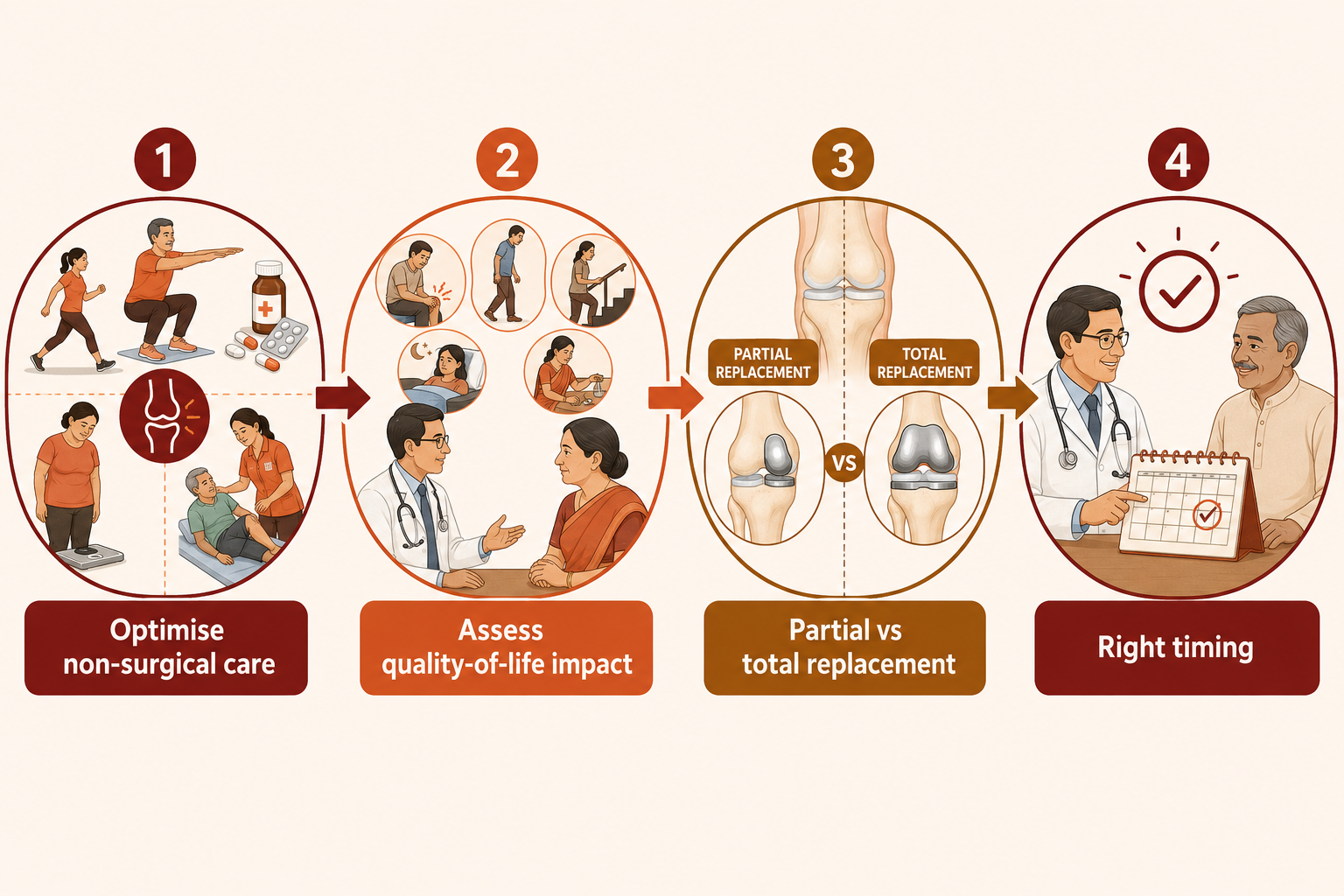
The choice is not simply surgery versus nothing — it is a spectrum:
1. Optimise non-surgical care first (for almost everyone):
2. Consider surgery when the above is no longer enough:
3. Timing. There is usually no emergency: replacing too early exposes you to surgery and a future revision you might have deferred; leaving it very late can mean more deformity and a harder recovery. The 'right time' is when the knee's impact on your life outweighs the downsides of surgery — a judgement made with you, not for you.
Outcomes are generally very good, but honest counselling covers that some stiffness or aching can persist and that implants do not last forever.
At VinayakM in Greater Kailash-1, this decision is guided by Dr Udit Vinayak, a trauma, sports medicine and joint replacement surgeon. Because he manages the whole pathway — not only the operation — the advice is balanced rather than surgery-first:
You should leave understanding your options well enough to make the decision with us — never feeling rushed into an operation.
You cannot always avoid needing a knee replacement, but you can often delay or reduce the likelihood, and make surgery safer if it comes:
Active management does not just postpone surgery; it means that, whenever it happens, you go in stronger.

The usual trigger is arthritis pain and stiffness that seriously limit your daily life — walking, stairs, sleep, independence — and that have not improved despite a genuine course of exercise, weight management, medication and sometimes injections. It is a decision based on your quality of life, made together with a surgeon, not on the X-ray alone.
Often, yes. Many people control arthritis symptoms for years with exercise, weight management, medication and injections. These measures can delay surgery and, if it is eventually needed, leave you stronger and fitter for it. Whether you can avoid it altogether depends on how the arthritis progresses.
Age alone rarely decides it. In younger patients, surgeons often try to defer replacement because implants do not last forever and a revision may be needed later. In older patients, general health and fitness for surgery matter more than the number itself. The decision is individual.
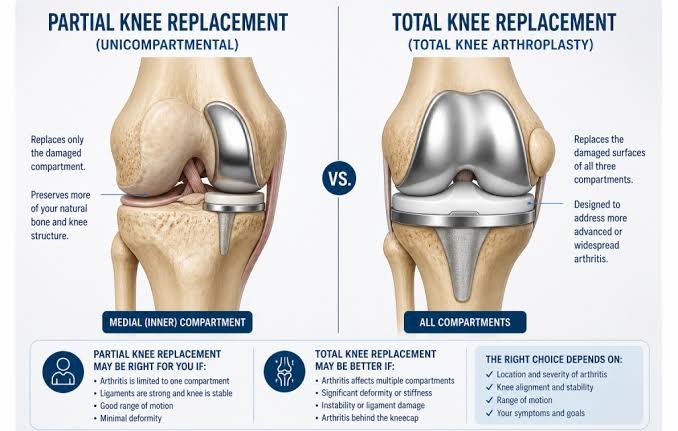
A partial (unicompartmental) replacement resurfaces only the worn part of the knee and suits selected patients with damage confined to one compartment, often with a quicker recovery. A total knee replacement resurfaces the whole joint and is standard when arthritis is widespread. Which is suitable depends on your knee.
Modern knee replacements last many years for most people, with a large proportion still working well more than a decade later. How long yours lasts depends on factors including your age, weight, activity level and the type of implant. Because they do not last forever, timing is part of the decision, particularly in younger and more active patients.
