
Articular cartilage is the pearly-white tissue, a few millimetres thick, that caps the ends of bones inside joints such as the knee, hip and ankle. It does two remarkable things at once: it makes joint surfaces more slippery than ice on ice, and it spreads load so that the bone underneath is not damaged by everyday impact.
Cartilage has an unusual biology. It contains no blood vessels and no nerves, and its cells (chondrocytes) are sparse and slow to divide. It is nourished mainly by joint fluid, which is pumped in and out as the joint moves — one reason movement is genuinely food for cartilage. The same biology explains its weakness: with no blood supply, cartilage cannot mount the healing response other tissues use, so significant damage tends to be permanent and can progress towards osteoarthritis over the years.
Understanding this one fact — cartilage protects you, but very little protects cartilage — is the basis of joint care at every age.

Cartilage problems are silent at first because cartilage itself has no nerve endings. Signs appear when damage affects the surrounding joint:
Because early damage is often silent, a history of joint injury — a twisted knee, a kneecap dislocation, a fracture into a joint — is itself a reason to look after that joint deliberately.
Cartilage is damaged in two broad ways:
Sudden injury (focal damage):
Gradual overload (wear-related damage):
Inactivity is also a cause: unloaded cartilage thins, because the fluid pumping that nourishes it stops.
See a doctor about a joint if:
Cartilage damage caught early, particularly in younger people, can sometimes be treated before it enlarges — late damage mostly cannot.
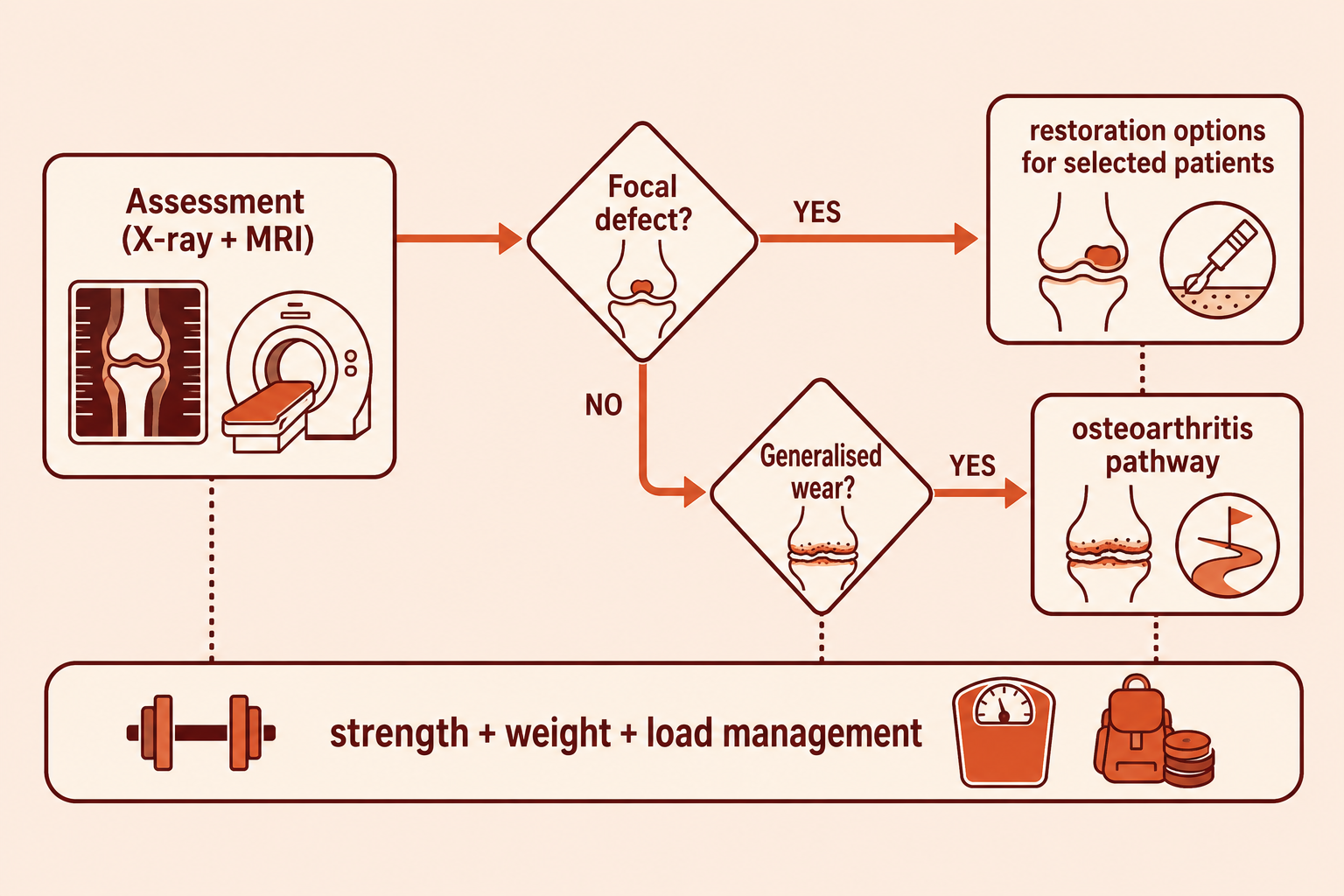
At VinayakM, assessment of suspected cartilage damage includes:
The assessment establishes whether the problem is a focal defect (a pothole in otherwise good cartilage — potentially repairable) or generalised wear (early osteoarthritis — managed differently), because the treatments are quite different.
There is no medicine that regrows cartilage. Honest treatment is about protecting what remains, and, in selected cases, surgically resurfacing a focal defect.
1. Protect and strengthen (everyone):
2. Symptom control:
3. Surgical options for focal defects (selected, usually younger patients):
Each option has specific indications, rehabilitation demands and honest limits — none recreates perfect native cartilage, and the right choice depends on the defect, your age, alignment and goals.
4. When wear is generalised, treatment follows the osteoarthritis pathway — see knee osteoarthritis.
At VinayakM in Greater Kailash-1, cartilage problems are assessed by Dr Udit Vinayak, trauma, sports medicine and joint replacement surgeon. That breadth matters for cartilage in particular, because the right answer spans the whole spectrum — from a physiotherapy-and-weight plan, through keyhole procedures for focal defects, to realistic advice when the damage is beyond repair. In practice:
The goal is decades more service from the joint you have.
Protecting cartilage is mostly about habits sustained over years:

Essentially no. Articular cartilage has no blood supply, so significant damage does not heal the way skin or bone does. Small areas can fill with a scar-like fibrocartilage, which is less durable than the original. This is why protecting cartilage — through strength, weight control and sensible loading — matters so much.
No supplement has been convincingly shown to rebuild cartilage. Trials of glucosamine and chondroitin show at best small, inconsistent effects on symptoms, and guidelines such as NICE do not recommend them. Exercise, muscle strength and weight management have far stronger evidence.
For most people with healthy joints, no — recreational running is not shown to wear out knees, and regular loading actually keeps cartilage nourished. Problems arise with sudden increases in distance, running through an injured or malaligned joint, or very high training volumes. Build up gradually and address pain early.
It is a localised area — like a pothole — where the smooth joint-surface cartilage has been damaged, often after an injury or kneecap dislocation, while the rest of the surface remains healthy. Focal defects behave differently from generalised wear and, in selected younger patients, can be treated with cartilage-restoration surgery.
Suspicion comes from the story: aching and swelling after activity, catching or clicking, or a past joint injury. Examination localises the problem, X-rays assess overall wear and alignment, and MRI is the test that actually shows cartilage. A normal X-ray does not exclude early cartilage damage.
No injection regrows cartilage. Some injections may ease symptoms in selected situations, but claims that an injection will restore your cartilage are not supported by evidence. Be cautious of any clinic promising cartilage regrowth.
